Note: For some time I’ve been meaning to write some notes up about how there all these different gaming communities. Each one is busy innovating in their own little world but not always fully aware of what is / has happened in the other communities. Some of these include: LARP, Megagames, BoardGames, UrbanGames, Alternative Reality Games, Corporate Games, Educational Games for Science, Escape Games, Immersive Theatre, Traditional Video Games etc. Clearly there are overlaps between some of these but with some many separate communities not all are in contact and fully understand what each other is doing. This was my first Megagame experience. I’ve been aware of them – but have never had the opportunity to play one (blame my little people). Fortunately, a good friend of mine Ben Green (along with Megagame designer Paul Howarth) developed a Hospital themed one and I was lucky enough to be invited along as an observer.
So what is a Megagame?
As with any group – communications become more complex and begin to break down as the size of the group increases. This is particularly problematic in multi-player games. For example, in the case of a typical turn based board game the more players we have, the less time each player has and the more complicated the game dynamics are. There is often an optimal number of players that create interesting dynamics while giving players a reasonable amount of time.
The Megagame movement attempt to solve this by creating games for player sizes of 40 right up to a few hundred. They address the issue of larger player numbers by having players form teams (or teams of teams).
Typically, the theme of the games have focused on politics, history and other conflicts. The earliest Megagames were played in the early 1980s and came out of war-gaming movement. For the past 40 years Megagames have continued with their own dedicated community and throughout this time have organised a few games each month. There are similar communities in North America and a handful across Europe.
Megagames Resurgence
Megagames have experienced somewhat of a resurgence in the last few years as a popular games podcast ‘Shut Up & Sit Down’ filmed their experience of playing Megagame ‘Watch The Skies’. A game likened to a Model UN where the countries of the world are preparing for an alien invasion.
If you’ve not seen that episode of ‘Shut Up and Sit Down’ it is available on YouTube here and is a great introduction:
EnTRUSTed Hospital Game (by Ben Green and Paul Howarth)
So in late July, I was invited to attend my first live Megagame experience in Manchester. I was fortunate that this experience would be a somewhat unusual Megagame as it is addressed the topic of running a hospital Trust.
We had a pre-game briefing on the afternoon before the main event where the teams were assigned, game mechanics explained and some game tasks began.

Co-game designers Paul and Ben introduce the game
Broadly speaking EnTRUSTed is a 40+ player Megagame where players are tasked with running a Hospital Trust – comprised of both a hospital and a board. Those players within the hospital must manage the day-to-day running of a hospital focusing on treating patients whereas the board deals with the higher level management issues and larger crises.
While it’s possible for these two groups to communicate directly it is mainly done through a mediating level – that of the middle-manager directorate level. The directorate players spend their time moving between the board and hospital sharing messages and information.
To give you an idea of what happens here are a few example tasks the board level had to deal with:
• handle the tasks sent down from the ‘Department of Health’
• review staffing policy
• deal with public relation issues
• create trust branding
• generate mission statements.

Heated debate in Sunrise Hospital Board
Whereas the hospital staff deal with:
• admitting patients
• treating their conditions
• managing those in the ICU (Intensive Care Unit)
• discharging patients to free up beds
The two areas are very much interlinked – so if the hospital performs well then they will be rewarded with tokens which can be passed up to the Board Level and can be used in a variety of ways such as to reduce the impact of the large crises.
The ‘Game Controllers’ (usually known as just controllers)
The game is ran or administered by a group of game controllers. Within Megagames controllers appear to be their chosen terminology as opposed to gamemaster (personally I’ve even used the term gamejockey). There were two controllers in each hospital, two in the puzzle room and one in each board room. In addition, the overall game designers are free to walk around and handle high level decisions. The individual controllers have a great deal of freedom to adapt their portion of the game and are provided with guidelines from the designer. The controllers talk about ‘reality over rules’ which gives them the flexibility to change things in response to player queries or actions.
Game Mechanics
If you’re not interested in the details of the game then feel free to skip this portion and jump straight to the ‘What I Learned’ bits. Or you can look at this handy diagram from Ben which explains the entire hospital patient game flow in a single diagram!
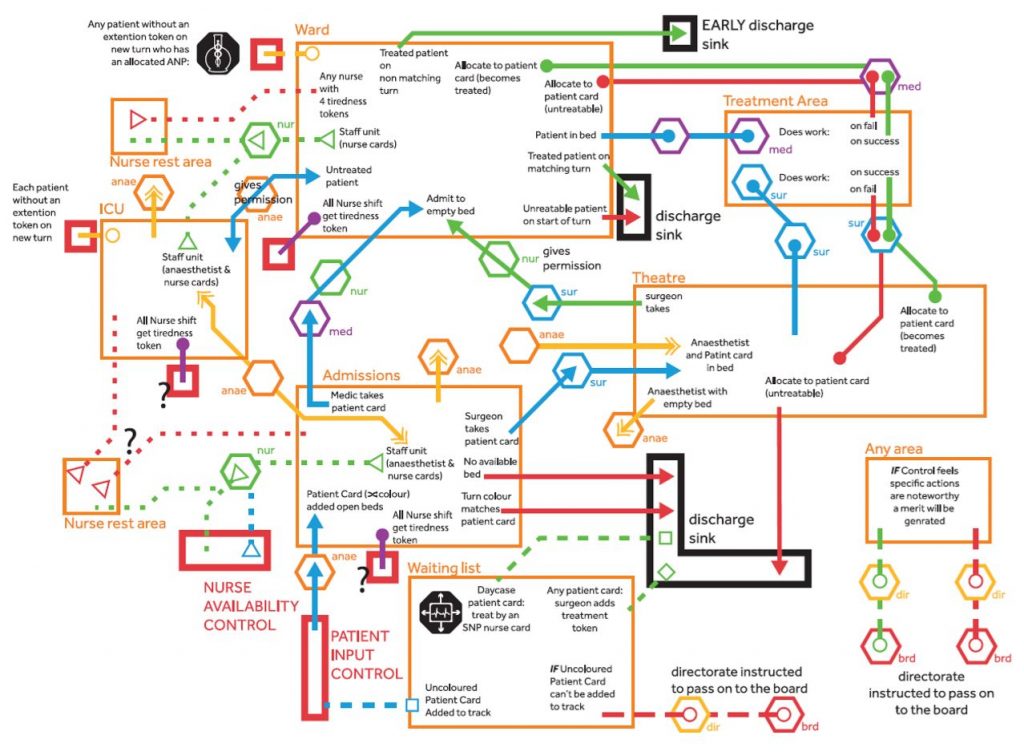
Detailed patient flow diagram illustrating movement of patients within the hospital system
So, probably my explanation is not really needed after that – but I’ll do my best to describe what I think happened 🙂 It’s worth knowing that nobody has a clear view of the entire game – even the controllers. Players and controller are generally focused on their own sub game within the overall larger game. It absolutely felt like a Megagame is a collection of several overlapping games which only a subset of players were involved in.
It’s quite possible to get through the entire experience and have a very selective view of what has happened. I think this is why it’s often common to include ‘Newspaper Reporter Player Role’ who go around speak to everyone and publish the main activities keeping everyone in touch with the wider stories.
Even though players have received training in the game mechanics – they are not expected to know them in detail as the controllers take care of that. It is common to hear players asking what happens in particular cases, if this is an unusual request then it might cause some discussion between the controllers.
A Game Turn (in the hospital)
 |  |
This is probably a good point to mention that there are two hospital trusts (each comprised of a their own board and hospital). All four of these operations take place in different rooms. The hospital rooms are large and contain many tables covered with game state / pieces (a bit like large board games). It’s fairly common in Megagames to have a central game state which certain players are permitted to examine and interact with. In a more traditional Megagame this would be a map of the world showing where troops, spies, bases are located.

Royal Red Brick Board present their new mission statement to ‘enthusiastic’ hospital staff!
I’ll talk about the hospital part in more detail than the Board as that aspect of the game is more about game systems. So these mechanics are somewhat familiar if you’re a player / maker of board games.
The hospital game is divided into turns of 10 minutes periods. You can see this within the hospital rooms as it is displayed on a large screen. The background colour indicates the current phase, the corner colours indicate the next phase and the timer provides an indication of time left for this turn. The phase colours have significance as they indicate which patients you can discharge. When patients arrive they have a colour associated with them, and they are only allowed to be discharged during a matching coloured phase. Actually, they are allowed to leave in different coloured phases but there could be additional penalties for this (as you’ve not allowed suitable patient recovery time).
Coloured phases of the game. Each turn advances this.
Beginning of a turn
At the beginning on each turn a new set of hospital patients arrive. This happens in two ways: via the waiting list or via admissions. The controller hands a batch of cards to an anaesthetist player handling the admissions. These patients can be randomly chosen or the controller has license to hand-pick easy / hard batches.

Latest patient arrivals being assigned to appropriate wards
Once they come through admissions – patients need to be assigned beds on a ward or in theatre. Patients are one of two types and have associated problems that are either medical or surgical.
Treating patients
Patients can be treated provided that they are in a bed on an appropriate ward and are accompanied by suitable medical staff: anaesthetists and nurses.
The process of treating patients involves the medic player solving mini-puzzles. A player in the medic role tells the hospital controller how many patients they wish to treat. The controller gives the medic a card with that number of patients on. This card is taken to the puzzle room where another controller provides the medic with a puzzle of corresponding difficulty. The puzzles are a series of popular off-the-shelf logic / spatial puzzles e.g. building a pyramid out of odd shaped blocks or the classic car-park challenge game.
 |  |
On completion of the puzzles medics return to the hospital with their successful treatment tokens (some times with failure tokens – based on how much help they might have needed with the operation). These tokens are placed on patients to indicate they had been successfully treated.
The idea of using logic puzzles to simulate ‘work tasks’ was really well-received. I always talk about how once you have established the goals of the game players are (somewhat surprisingly) usually willing to complete any task required – regardless of whether it appears to be connected with the theme of the game. Clearly, solving a logic puzzle has little in common with performing open-heart surgery but the players went with it very quickly.
These puzzles were also used when other challenges popped up – e.g. when it turned out that all staff needed retraining in GDPR – it was up to the directorate to ensure each player had been to the puzzle room to complete their ‘training’ puzzle.
Discharging players
Once players have been successfully treated they are eligible for discharge. As mentioned above a lot of this is down to the phase colour. Hospitals keep a tally of successful versus failed discharges.
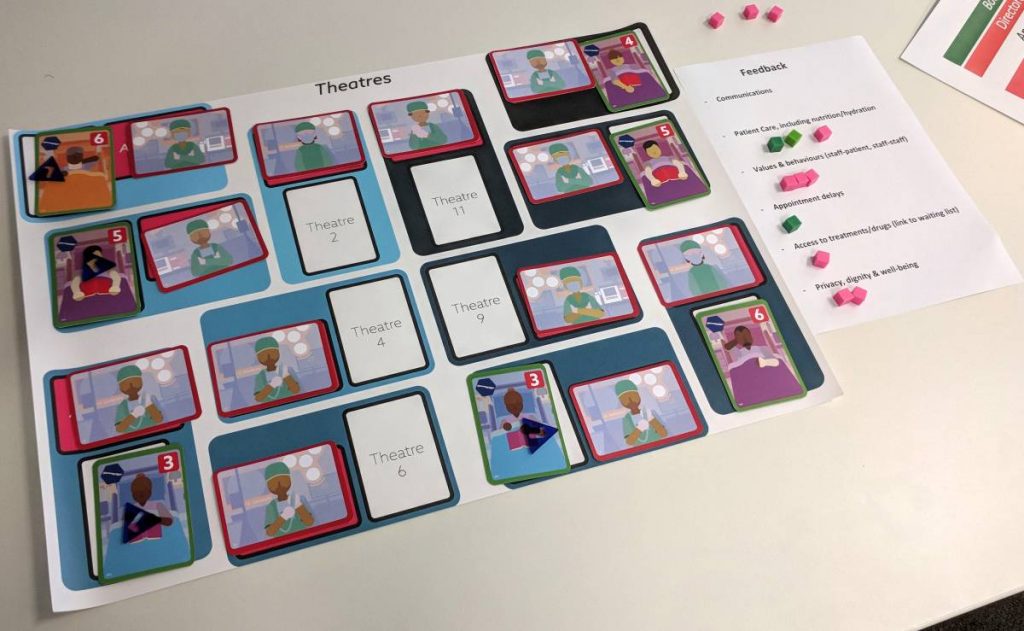
Well staffed theatres with beds available for more patients
End of Turn Clean-up
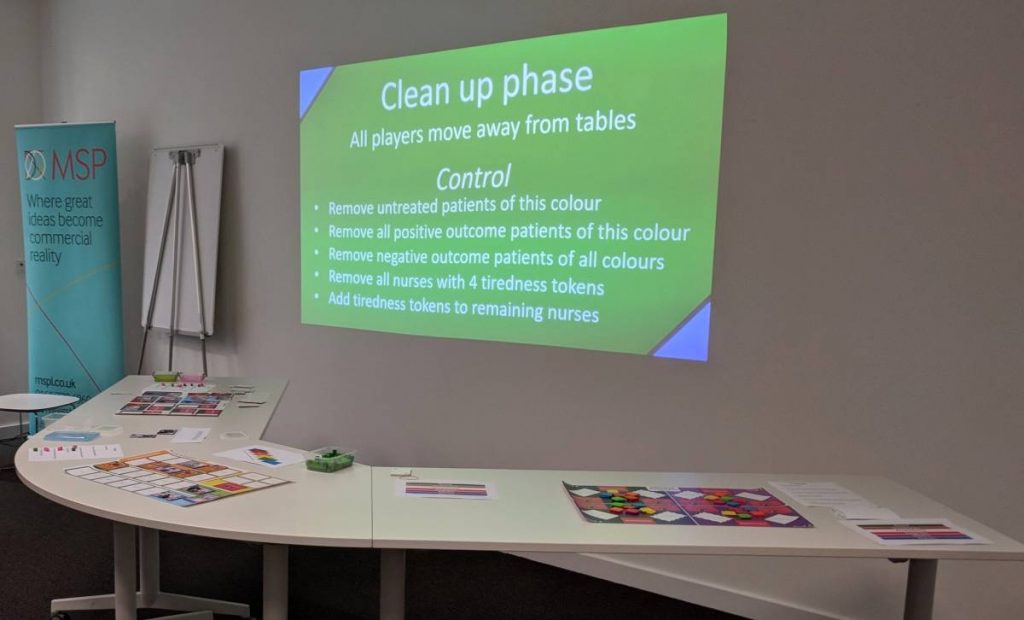
Controllers step-in during clean-up phase to update game state
Every 10 minutes a turn completes, players must move away from the tables and the controllers manually update the game state. Removing patients, rolling dice, adding tokens etc. This typically took 2 or 3 controllers 3-4 minutes.
Other Mechanics
Okay – this covers the absolute basics of the hospital. There are also game mechanics around nurse tiredness, staff morale, patient feedback, Intensive Care Unit, the use of wards and treating of patients on the waiting list. I suspect there are others that I’ve forgotten too – you can refer back to the exhaustive game flow diagram!
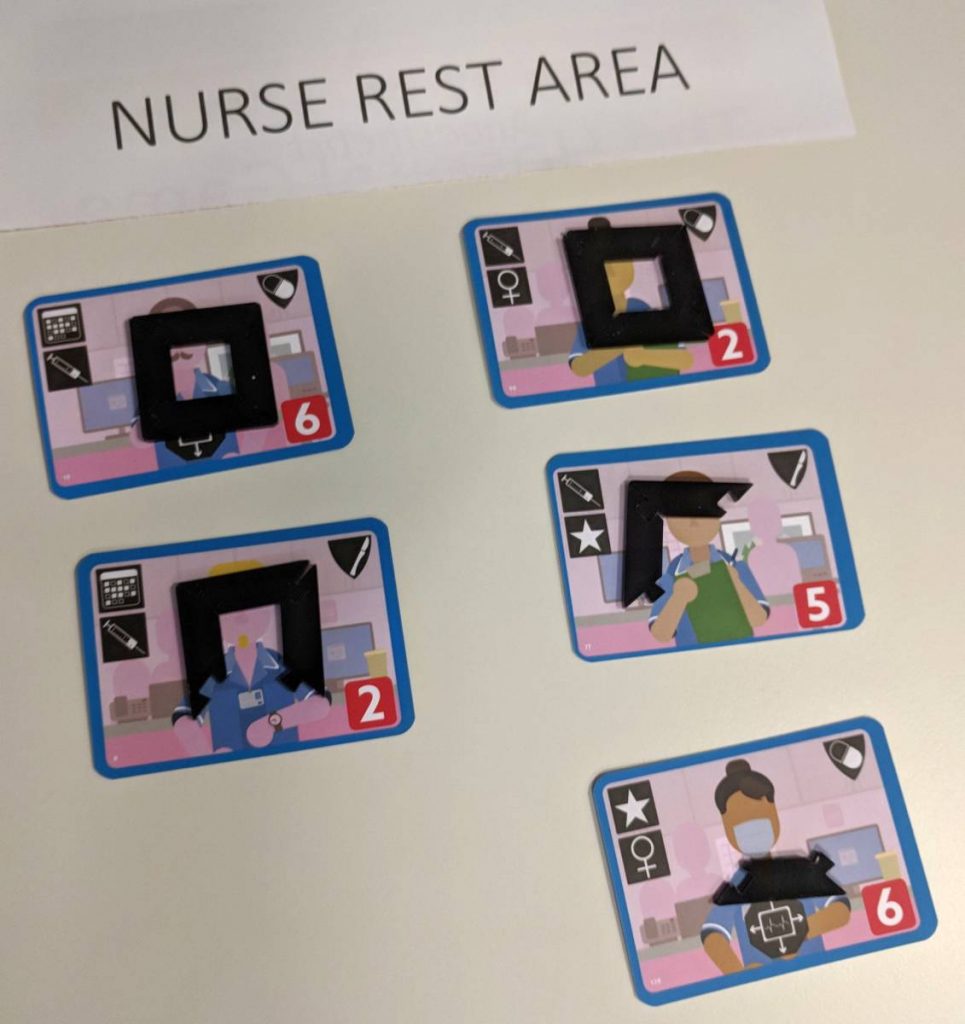
Nurses rest game mechanic. One tiredness token is removed each turn.
Game Balancing
What is interesting (as with large scale games that I’ve made in the past) it’s difficult to balance the game correctly. You can create simple simulations or the system – e.g. writing software or in excel. However, really the only way to test a game with 50 players is to have 50 players available for the playtest.
As you have a set of human game controllers – a big part of their role is to continually balance the game. They are able to look at the stress of the players and introduce more tasks or reduce the difficulty on the fly to ensure a great game experience.

Red Brick Hospital’s Expansion of ‘Megan’s Ward’ is accompanied via a Royal Visit
What I learned
I suspect that this wasn’t a typical Megagame with typical Megagame players. Predominantly Megagamers are male, the games often contain combat mechanics and the games difficulty increased by the controllers, so I suspect this leads to more volatile experiences (I’m not sure how to write that sentence to not include sweeping generalisations!). I think EnTRUSTed demonstrates that there is an appetite for more game types for more diverse audiences. As we’ve seen with the explosion of Escape Games to different audiences I think there is the potential for there to be Megagame-like experiences reach wider players. Perhaps they don’t run for entire days but I think the core idea of having many players collaborating in teams is interesting (and different enough from the current expansion of Escape Games into team based games).
Megagames are quite different to what I imagined. If you’ve seen the ‘Shut Up and Sit Down’ videos then it won’t come as a huge surprise that actually Megagames are more about role-playing and much less about the strategic decisions. When you know that the history of their origins and the topics – you’d expect the main game mechanics to be very strategy based. In fact it is nearly all about human interactions – players who performed best were those who were in constant communication.
The controllers were absolutely fantastic throughout! They were all very experienced players and controllers and were delighted to be sharing their passion with a new audience. The success of the game is a mix of the work up front by the game designers and the live running by the controllers. My feeling was that Ben and Paul had managed to assemble pretty much a dream team of controllers. They were constantly looking to make minor tweaks to the game to improve it and always looking to engage the players in fun and interesting ways.
There are no winners. As with (Nordic) LARP or other forms of Role-Play it’s really about having a shared experience in a shared make-believe world. Controllers adjust the level of difficulty or introduce additional challenges in response to how the players are performing. I suspect that because we had a good ratio of controllers to players this was managed very well. Just as in the games I make I am all for emphasising the experience over the outcome. Perhaps in more traditional Megagames the outcome is more important.
The use of hidden information worked wonderfully. The hidden information mechanic is a great one and simply by limiting who is allowed to view the central hospital game state you introduce lots of interesting human complexity between sub-teams.
The mini-puzzles were hugely popular. I think it was largely due to the excellent assistance and role-playing from John & Les in the puzzle team. They did a grent job of providing subtle hints without penalising the players. It’s often the case that some players hate logic puzzles – so giving them a series to complete results in poor player enjoyment. The medic players were super engaged to the point they were running back and forth between the puzzle room and their hospital and would often collaborate when solving tasks.
What Next?
Huge thanks to Ben for inviting me along and letting me observe my first Megagame in the flesh, co-game designer Paul and the team of controllers (mostly called John – although they also included a Hugo, Phil, Andy, Les and Pete).
Massive congratulations to Ben, Georgina Moulton, Vicky Turner and everyone at the Health e-Research Centre & The Farr Institute of Health Informatics Research for attempting something so innovative. It’s my understanding that there will be a video made from the days. Although judging by the volume of footage recorded during the event it might take a long time to edit it down!
I hope that more information will be shared from the day as I think EnTRUSTed makes a very strong case for the use of Megagames in other scenarios.